 vs Top Alternatives: A Detailed Comparison")
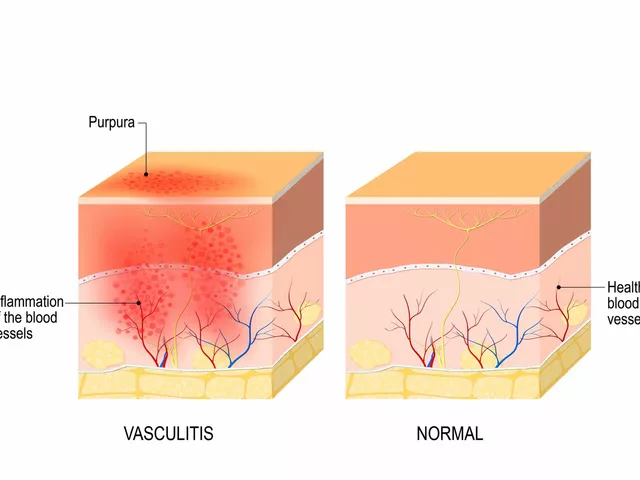
When it comes to allergy relief, Flonase nasal spray is a prescription medication that delivers fluticasone propionate, a corticosteroid that reduces nasal inflammation and congestion, a go‑to for many dealing with allergic rhinitis.
Fluticasone, the active ingredient in Flonase, binds to glucocorticoid receptors in the nasal mucosa. This blocks the release of inflammatory mediators like histamine, leukotrienes, and prostaglandins. The result is less swelling, fewer mucus secretions, and clearer breathing within 12‑24 hours of the first dose.
Because it’s a steroid, Flonase is classified as a prescription‑only product in the U.S., though many pharmacies carry it over the counter after a pharmacist consultation.
Several other nasal sprays aim at the same symptoms, each with its own chemistry and usage profile.
| Product | Active Ingredient | Prescription? | Onset (hrs) | Duration (hrs) | Typical Monthly Cost (US$) | Common Side Effects |
|---|---|---|---|---|---|---|
| Flonase | Fluticasone propionate | Yes (OTC after pharmacist consult) | 12‑24 | 24 | 15‑20 | Nosebleeds, throat irritation |
| Nasacort | Triamcinolone acetonide | No | 12‑24 | 24 | 12‑18 | Dryness, mild nosebleeds |
| Rhinocort | Budesonide | Sometimes (OTC in some states) | 12‑24 | 24 | 13‑19 | Headache, sore throat |
| Dymista | Azelastine + Fluticasone | Yes | 1‑2 (antihistamine) + 12‑24 (steroid) | 24 | 30‑35 | Bitterness, drowsiness |
| Saline spray | Sterile saline | No | Immediately | Variable (depends on usage) | 5‑10 | None (rare irritation) |
| Cetirizine (oral) | Cetirizine | No | 1 | 24 | 10‑12 | Sleepiness (low dose), dry mouth |

If you need strong, long‑lasting control of nasal inflammation, Flonase often edges out its rivals. Its high receptor affinity translates to consistent reduction of swelling, especially for people with chronic allergic rhinitis or mild nasal polyps. Because it’s a single‑ingredient steroid, you avoid the taste‑related complaints sometimes reported with antihistamine‑steroid combos like Dymista.
People who have tried multiple OTC sprays and still experience breakthrough congestion often find Flonase the upgrade they need.
Every nasal spray has a sweet spot. Below are scenarios where switching makes sense.
In practice, many clinicians start patients on an OTC steroid like Nasacort, then step up to Flonase if symptom control remains inadequate.

All steroid nasal sprays share a risk profile, but the severity varies with usage patterns.
There’s no one‑size‑fits‑all answer. If you crave the strongest, longest‑lasting anti‑inflammatory punch and don’t mind a prescription, Flonase is the front‑runner. If cost or OTC access matters more, Nasacort or Rhinocort give you similar relief at a lower price. When you need instant itch relief on top of inflammation control, Dymista’s combo shines. And for those who prefer a pure, drug‑free approach, saline spray is a safe daily habit.
Talk to your pharmacist or physician about your symptom pattern, any existing health conditions, and your budget. Most experts recommend trying an OTC steroid first, then moving to a prescription if needed. Whatever you choose, proper spray technique and adherence to dosage will make the biggest difference in how quickly you breathe easy again.
Most users notice reduced congestion within 12‑24 hours of the first dose, with full anti‑inflammatory effects building over a few days of regular use.
Yes. Combining a steroid nasal spray with an oral antihistamine like cetirizine can target both inflammation and histamine‑driven itching, providing broader relief.
Flonase is approved for children 4 years and older, but pediatric dosing is usually half the adult dose. A doctor should monitor growth if used long‑term.
Dymista adds azelastine, an antihistamine that starts relieving itching within minutes, so it’s ideal for people who experience intense sneezing or itchy eyes alongside congestion.
Saline helps clear allergens and moisturize the lining but doesn’t reduce inflammation. It’s best used as a complementary rinse, not a full replacement for steroids when you need anti‑inflammatory control.



12 Responses
Flonase does the job but you still need to watch the dosage; two sprays per nostril is the sweet spot. Overusing it can lead to persistent dryness and occasional nosebleeds, which some folks find annoying. Keeping the spray angled away from the septum helps minimize irritation.
For people on a budget, Nasacort offers almost the same anti‑inflammatory punch without a prescription. The price difference can add up over months, especially if you’re using daily. Also, the dosing schedule is identical – two sprays per nostril once a day – so the switch is painless.
Saline spray is a solid daily routine, it clears out pollen and keeps the lining moist.
When it comes to pharmacodynamics, fluticasone’s receptor affinity exceeds that of triamcinolone, which translates into a slightly longer half‑life in the mucosa. That’s why some patients notice steadier control with Flonase. Dymista throws an antihistamine into the mix, giving rapid itch relief alongside the steroid’s anti‑edema effect 😊. If you’re juggling both congestion and sneezing, the combo can be a game‑changer.
Flonase is pricey but works.
Proper technique matters a lot; aim the nozzle toward the outer wall of the nostril, not straight up the septum. This reduces the risk of local irritation and nosebleeds. Also, prime the pump a few times before first use to ensure consistent dosing. If you notice any crusting, a quick rinse with sterile saline can help.
Wow, thanks for the tutorial, Brad. I guess most of us just spray and hope for the best, huh? Maybe next time we’ll actually read the label.
Cost is a real hurdle; Flonase can set you back twenty bucks a month, while Nasacort often slides under fifteen. If you’re not covered by insurance, those extra fees add up quickly. That’s why many folks start with the cheaper OTC option before going prescription.
Choosing a nasal spray is ultimately a personal balance between efficacy, side‑effects, and budget. One must weigh the long‑term benefits against the immediate cost.
Sarah makes a solid point about balancing cost and results. It’s like picking the right tool for a garden; you don’t need a chainsaw for a tiny hedge. Find what works for you and stick with it.
From a pharmacoeconomic perspective, the choice between Flonase, Nasacort, and Rhinocort can be framed as a cost‑effectiveness analysis over a defined treatment horizon. Fluticasone propionate, the active agent in Flonase, demonstrates a marginally higher receptor binding affinity compared to triamcinolone acetonide in Nasacort, which may translate to a modest improvement in symptom control for severe allergic rhinitis. However, the clinical significance of this difference is often outweighed by patient adherence factors, such as ease of access and out‑of‑pocket expense. The average monthly cost of Flonase, ranging from $15 to $20, exceeds that of Nasacort, typically priced between $12 and $18, by a small yet perceptible margin. When budgeting for chronic therapy, this differential can accumulate to several hundred dollars annually, a consideration for uninsured or underinsured populations. Moreover, the safety profile of intranasal corticosteroids remains favorable across the board, with the most common adverse events being local irritation, epistaxis, and mild headache. Long‑term data suggests no systemic glucocorticoid effects at recommended doses, though pediatric monitoring is advisable. In practice, many clinicians adopt a step‑wise approach: initiate therapy with the least expensive OTC steroid, assess symptom control, and only then consider escalation to a prescription‑only formulation or a combination product such as Dymista. Dymista’s dual mechanism, incorporating azelastine hydrochloride, offers rapid antihistamine action alongside the steroid’s anti‑inflammatory effects, but it carries a higher price tag, often exceeding $30 per month. For patients with predominant itch and sneezing, the added benefit may justify the cost, whereas those with primarily congestion may find a single‑agent steroid sufficient. Saline irrigation, while ineffective for reducing underlying inflammation, serves as an adjunctive measure to clear particulate matter and improve mucociliary clearance; its negligible cost makes it a universally acceptable recommendation. Ultimately, the optimal choice hinges on individualized assessment of symptom pattern, financial constraints, and patient preference, underscoring the importance of shared decision‑making in allergy management.
Great summary, Larry. I’d add that trying a saline rinse before any spray can improve comfort and reduce the needed dose. Keep up the good work!